
Preventing Readmissions and Reducing Utilization of Unnecessary Services
By Ivy Xiwen Deng
Data Visualization by Sanat Malhotra
In the wake of the Affordable Care Act (ACA), hospitals have drawn attention from policymakers as key partners in reducing the overall cost of care. Consequently, the effort has led to an enhanced focus on preventing readmissions and reducing unnecessary care.
The ACA implemented several policy measures to hold hospitals accountable for what happens to patients post-discharge. For example, the Hospital Readmissions Reduction Program, Bundled Payment for Care Improvement Initiative (BPCI), and Comprehensive Care for Joint Replacement (CJR). Such models aim to incentivize hospitals to be more proactive in impacting patient outcomes and reducing a patient’s overall cost of care. The Improving Medicare Post-Acute Care Transformation Act of 2014 (IMPACT Act) mandates data submission of standardized patient assessments, quality measure, and resource use by post-acute care providers (PAC). The Act targets improvements in care coordination and communications to lower the cost of care.
Finding the Gaps with Data
Despite the emphasis placed on these efforts, significant knowledge gaps persist in assessing the variations and obstacles within post-acute care systems, including skilled nursing facilities (SNF), home health agencies (HHA), hospices, rehabilitation hospitals, and long-term hospitals. CareJourney data show that, in 2018, on average, almost half of Medicare patients discharged from inpatient short-term acute care hospitals went directly home.
Hospital discharge patterns vary dramatically by facility (see figure below). Based on data pulled from CareJourney’s Healthcare Analytics Platform, in 2018, 73.25% of inpatient short-term acute care facilities discharged less than 50% of their Medicare Fee-for-Service (Medicare FFS) patients to any post-acute settings. 26.75% of facilities discharged at least 50% of their Medicare FFS patients to post-acute facilities.
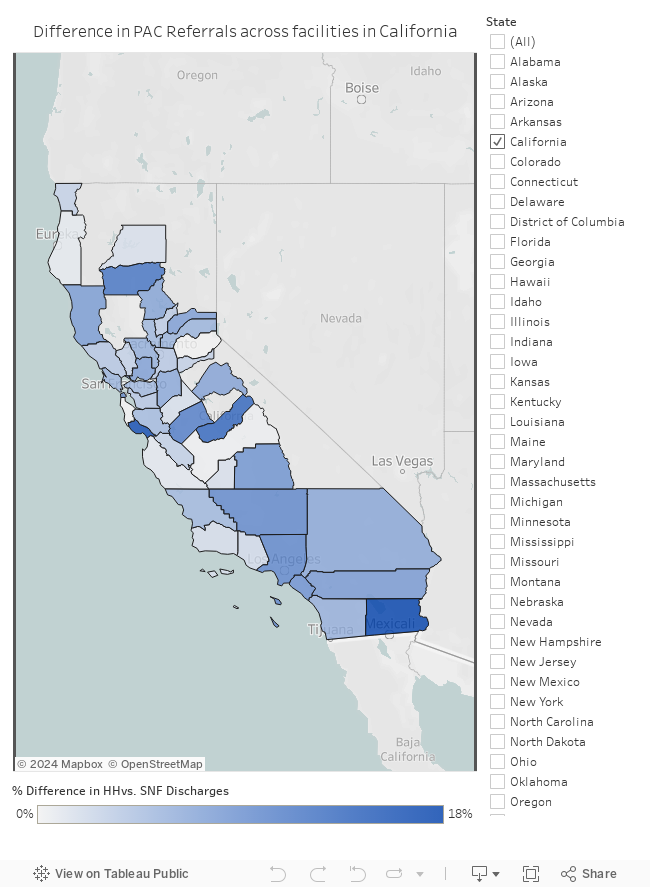
Further, our data indicate that among patients who were discharged to post-acute facilities, over half of the patients were referred to SNFs, and more than one-quarter of the patients were discharged to HHAs. A study conducted by the Institute of Medicine (IOM) finds that geographic variation in Medicare expenditures is largely attributed to post-acute spending.i SNFs also account for the most substantial portion of post-acute spending, compared to the expenditures of other post-acute facilities. The total allowed amount of SNFs in 2018 topped $18.4 billion, almost twice the total allowed amount of HHAs.
While the Medicare system offers patients various kinds of post-acute care options, the challenge patients and providers encounter when choosing the “best fit” remains. It is not only about “which type of post-acute care should the patient go,” but also about the lack of evidence-based methodology to determine the best option for the particular patient. For example, an American Journal of Surgery study shows that for patients discharged after abdominal surgeries, potential cost savings from increasing referrals to HHAs instead of SNFs/IR were from $2.5 to 438 million annually.ii In contrast, other researchers argue that among Medicare patients eligible for post-acute both at HHAs and SNFs, discharge to HHAs was associated with higher rates of readmission.iii
Moreover, financial incentives – such as a readmission penalty – don’t always lead to better patient outcomes. The Center for Medicare and Medicaid Services (CMS) data for the fiscal year 2019 suggest that 73% of SNFs enrolled in the Skilled Nursing Facility Value-Based Purchasing Program will be penalized on their Medicare payments for poor readmission rates. According to a Modern Healthcare article, the longer time a SNF has been in the program, the worse they perform at lowering readmission rates.iv
Marketing Intelligence You Need
CareJourney’s Healthcare Analytics Platform provides the market intelligence that users need to understand the variation in post-acute referrals and to pinpoint how different post-acute providers impact quality and overall cost. Learn more by requesting a demo below.
Build and Optimize Networks of Care with Network Advantage
REQUEST A DEMO
i Institute of Medicine. 2013. Variation in Health Care Spending: Target Decision Making, Not Geography. Washington, DC: The National Academies Press. https://doi.org/10.17226/18393.
ii Balentine CJ, Leverson G, Vanness DJ, et al. Selecting post-acute care settings after abdominal surgery: Are we getting it right? The American Journal of Surgery. 2018;216(2):260-266. doi:10.1016/j.amjsurg.2017.08.043
iii Werner RM, Coe NB, Qi M, Konetzka RT. Patient Outcomes After Hospital Discharge to Home With Home Health Care vs to a Skilled Nursing Facility. JAMA Intern Med. 2019;179(5):617-623. doi:10.1001/jamainternmed.2018.7998
iv Castellucci M. Most skilled-nursing facilities penalized by CMS for readmission rates. Modern Healthcare. November 2018. https://www.modernhealthcare.com/article/20181128/NEWS/181129930/most-skilled-nursing-facilities-penalized-by-cms-for-readmission-rates. Accessed October 7, 2019.