
BASIC
Benchmarking Analysis on Segments for Improved Care
Learn how BASIC can help identify performance gaps in your ACO’s operating costs.
Pricing available upon request.
An Open, Research-Led Effort to Boost ACO Performance
Published evaluations of CMS MSSP performance have shown modest results, and factoring in operating costs to achieve them, a net loss to the majority of ACO operators.
Harvard Professor Ashish Jha is anchoring a newly proposed research network to help address this performance gap by developing clinically-meaningful patient segments, benchmarks, and peer-reviewed methodologies for rapid adoption and use.
CareJourney has agreed to serve as a “partnering data firm” connecting any interested member’s CCLF files for analysis in exchange for personalized benchmarks that:
- Help ACOs better understand their patients by benchmarking segment mix to peers
- Identify opportunities for high need, high cost (HN/HC) segments such as managing preventable spend
- Facilitate rapid hypothesis testing and evaluation by Professor Jha’s research team.
CareJourney offers this service as part of its annual membership, but will extend provision of these services to any ACO for a nominal fee to cover data processing and insights report production.
The National Academies of Medicine incorporated this segmentation work as foundational for its activities targeting high-need, high-cost patients.
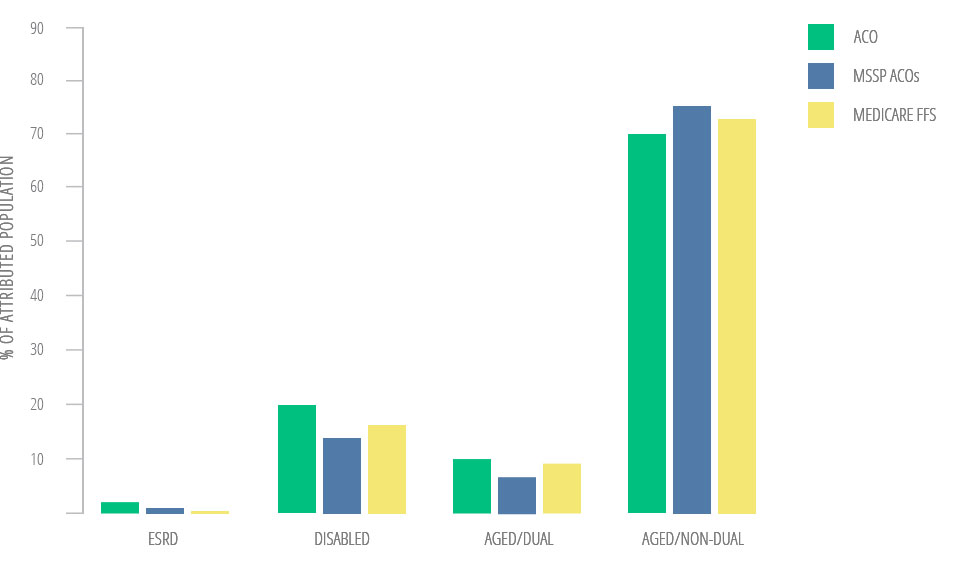
Beneficiary Segmentation for MSSP ACO
CMS provides benchmarks across four distinct categories
ACO Population Mix
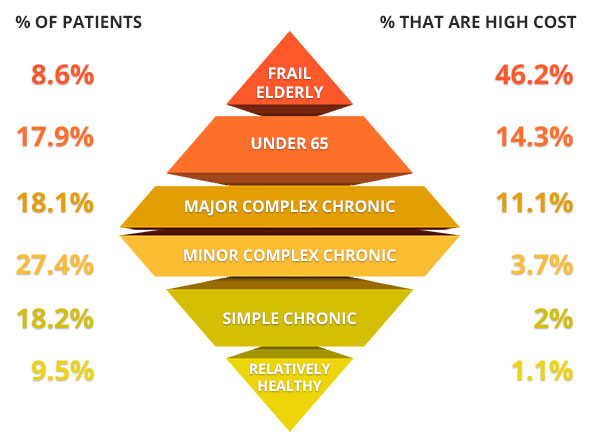
Prof. Jha Finds Clinically Meaningful Segments
As prelude to research initiative, methodology is peer-reviewed and open
ACO Population Mix

Joynt, K.E., Healthcare (2016), http://dx.doi.org/10.1016/j.hjdsi.2016.11.002
Segments defined
Frail elderly:
Age age ≥65 and the presence of at least two conditions on a modified list of twelve specific claims-based diagnoses potentially indicative of frailty (gait abnormality, malnutrition, failure to thrive, cachexia, debility, difficulty walking, history of fall, muscle wasting, muscle weakness, decubitus ulcer, senility, or durable medical equipment use)
Under 65 ESRD and disabled:
The under-65 Medicare population, which consists of those qualifying for Medicare based on the presence of end-stage renal disease (ESRD) or disability as determined by the Social Security Administration
Major complex chronic*:
Two or more complex conditions or at least 6 non-complex conditions
Minor complex chronic*:
Only 1 complex condition and less than 6 non-complex conditions
Simple chronic*:
1-5 non-complex chronic conditions
Relatively healthy:
All others not captured by the above 5 categories
*The researchers started with the list of 29 key chronic disease outlined by CMS in their measure for unplanned admissions for patients with multiple chronic conditions. They defined 9 conditions as “complex conditions:” Acute Myocardial Infarction / Ischemic Heart Disease, Chronic Kidney Disease, Congestive Heart Failure, Dementia, Chronic Lung Disease, Psychiatric Disease, Specified Heart Arrhythmias, Stroke, and Diabetes. They defined the remaining 20 conditions as “other non-complex conditions.”
CareJourney Maps Spend by Patient Segment
Enables more robust benchmarks across cohort
ACO Spend

Joynt, K.E., Healthcare (2016), http://dx.doi.org/10.1016/j.hjdsi.2016.11.002
Patient Segmentation “Diamond”
Frail elderly disproportionately account for HN/HC beneficiaries
Joynt, K.E., Healthcare (2016), http://dx.doi.org/10.1016/j.hjdsi.2016.11.002
Preventable Spend
A focus on HN/HC patients reveals high preventable spend in IP setting
ACO Preventable Spend
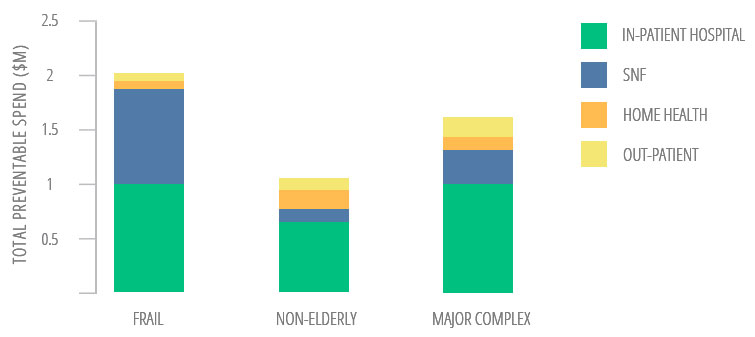
Figuerora, et. al., Concentration of Preventable Spending Among High-Cost Medicare Subpopulations
